Bulletin: Composed Classifiers
Introduction
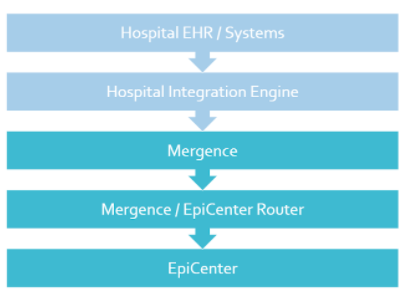
All Emergency Department Registration data coming into EpiCenter is automatically classified by the system. Classifications are categories or tags associated with each healthcare interaction that are used by EpiCenter’s Syndromic Surveillance and other analyses. Classifiers are groupings of conceptually similar classifications.
Classifications for Acute Care Interactions are based on an individual data field. Most commonly this is the “chief complaint” field, but others such as diagnosis code can be considered as well. Health Monitoring also supports the definition of “composed classifiers”, which combine evidence across multiple classifications. This bulletin provides more detail about composed classifiers and how they work.
Details of Clarification
Evidence Classifications
EpiCenter’s system classifications for acute care interactions are based on individual, discrete pieces of evidence. Many classifications are based on chief complaint, medical notes, or observations, all of which are free-text fields. Classifications based on free-text fields are defined by the inclusion of one or more words or phrases and an optional list of negative words or phrases. If an interaction’s text field matches the definition of the classification, the classification will be tagged to the interaction. An interaction can have multiple classifications from multiple classifiers applied to it.
To use a simplified example, the “Suicidal Ideation” chief complaint evidence classification searches for chief complaints that include the word “suicide” but not the phrases “denies self-harm” or “accident.”
Other classifications are based on diagnosis code. Instead of parsing a free-text field, these classifications simply search for a specific diagnosis code or codes. For example, the “Flu Diagnosis” evidence classification looks for ICD9 or ICD10 codes corresponding to influenza.
Composed Classifiers
Composed classifiers are based on multiple pieces of evidence, using combinations of classifications. Composed classifiers can use the logical operations AND, OR, and NOT.
For example, the “Suicidal Ideation” composed classifier looks for interactions tagged with either the “Suicidal Ideation” chief complaint evidence classification described above, OR the “Suicidal Ideation” classification based on diagnosis code OR the “Suicidal Ideation” classification based on text evidence found in medical notes.
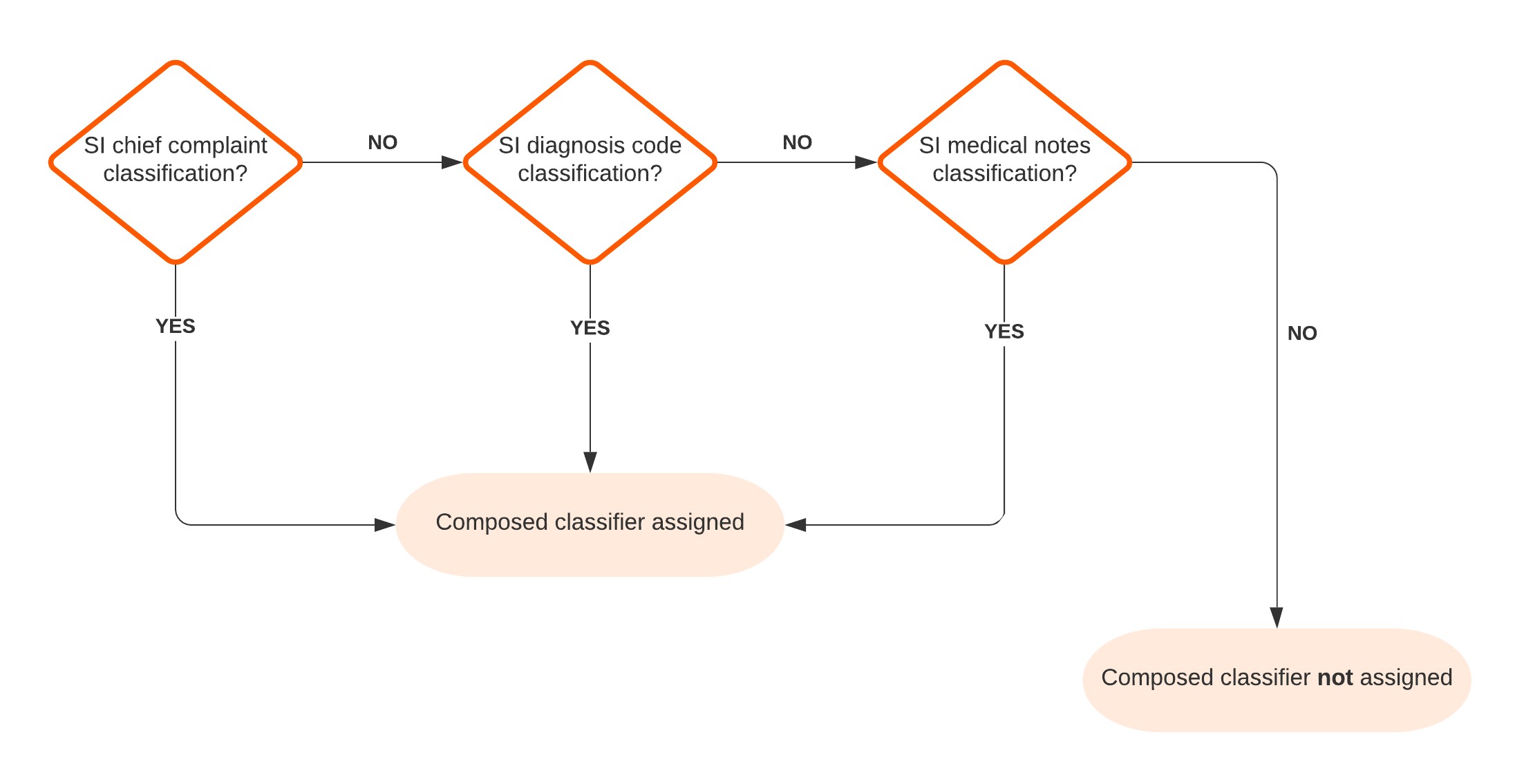
Figure 1 – Suicidal Ideation Composed Classifier Flow Chart
As another (simplified) example, the “COVID-19 Symptoms (Broad)” composed classifier looks for interactions tagged with EITHER the “COVID-19” diagnosis evidence classification OR a “Fever” classification from chief complaints, medical notes, or vital signs AND at least one of a “Cough” or “Dyspnea” classification from chief complaints or medical notes AND NOT an “Influenza” diagnosis classification.
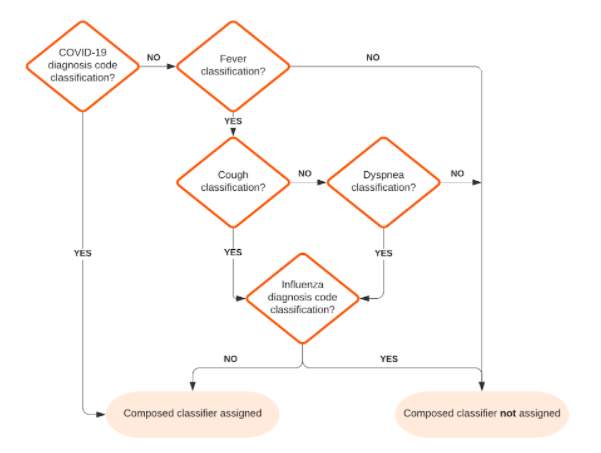
Figure 2 – Simplified COVID-19 Symptoms (Broad) Composed Classifier Flow Chart
Impact
No changes are planned to existing system classifiers or classifications. Development of new composed classifiers can be supported as a customization.